During pregnancy, routine ultrasounds are vital for monitoring the health and development of the fetus. One important scan is the anomaly or anatomy scan, generally performed between 18 and 20 weeks gestation. This specialised ultrasound evaluates various aspects of fetal development, including the kidneys. Occasionally, during this scan, the renal pelvis—the area where the ureter connects to the kidney—may appear dilated, a condition known as urinary tract dilation. Know more regarding this condition from the doctors specialising in fetal medicine.
What is Urinary Tract Dilation?
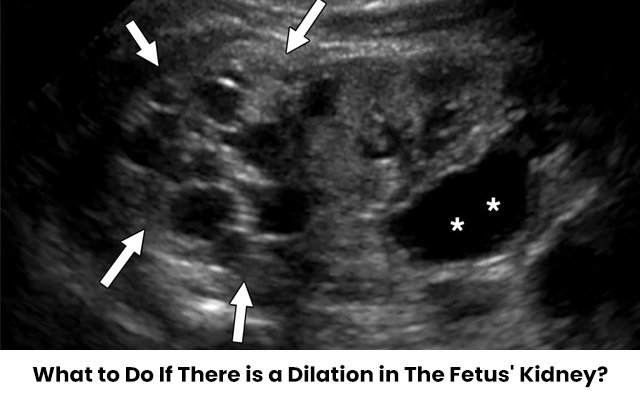
Urinary tract dilation occurs when there is an abnormal enlargement of the renal pelvis. This condition can be detected when the diameter of the renal pelvis is greater than expected. Normally, during pregnancy up to the 27th week, this distance should be less than 4 mm. If the dilation exceeds this measurement, it may indicate an issue that requires further investigation.
Urinary Tract Dilation (UTD) is a common finding and can vary in severity. Mild dilation, known as UTD A1, is characterized by a measurement between 4 and 7 mm. While this may be a marker for conditions such as Down syndrome, it requires only routine follow-up ultrasounds. Severe dilation, termed UTD A2-3, measures between 7 and 11 mm and may pose a higher risk of kidney damage or hydronephrosis.
Causes and Implications
Several factors can cause urinary tract dilation:
- Obstruction: Blockages at various sites in the urinary tract, such as at the uretero-pelvic junction (where the ureter joins the kidney), uretero-vesical junction (where the ureter joins the bladder), or at the vesico-urethral junction (where urine exits the bladder) can lead to dilation.
- Implications: If urine flows back into the kidney instead of exiting through the bladder, it can cause dilation of renal pelvis and eventually calyces which may lead to potential damage to the kidney.
Management During Pregnancy
During pregnancy, managing urinary tract dilation primarily involves regular monitoring by doctors specialising in fetal medicine If dilation is detected, your doctor will schedule follow-up ultrasounds every 4 to 6 weeks to track the condition’s progression. The goal is to assess whether the dilation is increasing and to evaluate if the kidney is being affected. In most cases, dilation does not lead to significant complications, but close monitoring is essential to catch any potential issues early.
Post-Birth Evaluation and Treatment
After birth, a paediatric nephrologist will evaluate the infant’s condition. If the dilation is severe or if there are signs of kidney damage, immediate treatment may be necessary. Newborns with significant urinary tract dilation might be at risk for urine infections or other complications, so it’s important to inform the neonatologist of the condition. Immediately, after birth, antibiotic drops are given if needed.
Following this, treatment options vary depending on the severity of the dilation:
- Mild Cases: Often managed with observation and follow-up scans to ensure the condition does not worsen.
- Moderate to Severe Cases: May require interventions after 3 months of the baby’s birth such as a radionuclide scan to assess kidney function, and in some cases, surgery to correct the obstruction.
In rare cases where dilation is detected early in pregnancy (within 3 months) , interventions may include in-utero procedures to relieve the obstruction or, if the damage is irreversible, termination of pregnancy may be considered. However, this is a rare occurrence.
Conclusion
Urinary tract dilation detected during an anomaly scan can be concerning. Regular monitoring and consultation with doctors specialising in fetal medicine help ensure that any potential issues are managed appropriately, providing the best outcome for both mother and baby.
If you receive a diagnosis of urinary tract dilation, work closely with your doctor to develop a comprehensive management plan and address any concerns you may have.